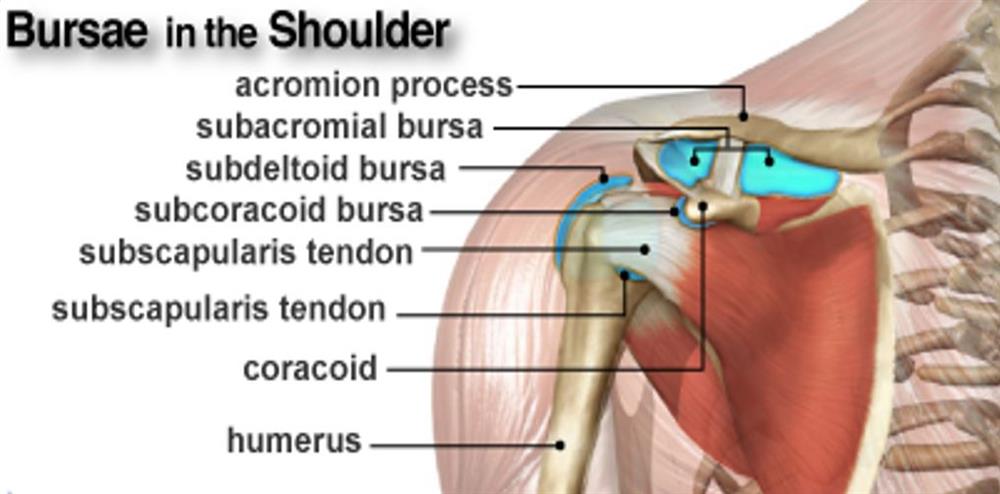

Shoulder bursitis is a painful condition resulting from inflammation to the bursae of our shoulder. Bursae are a fluid filled sac which can be found surrounding joints and bony prominences all over our body. They facilitate movement by acting as a cushion to reduce the friction between tendons, ligaments and bone. The main shoulder bursae are:
The sub-acromial bursa is the most affected bursa of the shoulder. In shoulder bursitis, the bursa is compressed during shoulder elevation, between the acromion process and either the rotator cuff tendons, humeral head or coraco-acromial ligaments.
Shoulder bursitis is closely related to the condition shoulder impingement (hyperlink to impingement article) as any kind of impingement in the shoulder will likely result in compression of the bursa.
Most cases of shoulder impingement present as chronic, overuse type injuries. This form of bursitis is common in those who perform repeated overhead such as painters, tennis players or basketballers. Certain biomechanical factors may be present which predispose individuals to developing bursitis and the reason why the pain does not go away. These factors may include:
Less commonly, bursitis can present as an acute injury. This may result from a fall or direct trauma to the shoulder. This could be seen in the elderly population after a fall, racquet athletes or in contact sports. It is important in these cases that fractures, rotator cuff tears and dislocations are first excluded before proceeding with treatment.
Typically, people complain of pain in the front or outside of the shoulder, which may extend as low as the elbow.
As many cases are in part due to overuse, onset of shoulder pain may begin as a dull ache when lifting the arm. Gradually over the coming weeks to months, this pain may worsen, becoming more consistent and possibly associated with a loss of strength or range of motion.
Activities involving raising the arm such as combing your hair, hanging out washing or reaching to the top cupboard aggravate symptoms. Laying on the affected arm may also aggravate the symptoms.
The painful arc, as pictured below, is a key sign of shoulder bursitis. This is where pain is at its worst approximately between 60-120 degrees of shoulder elevation, and above this range pain is alleviated. This is due to the pressure that is placed on the bursa through this range, as the arm is raised further and pressure is lessened, pain subsides.
Physiotherapy is highly indicated for diagnosing and treating shoulder bursitis. The early stages of Physiotherapy therapy treatment will aim to alleviate the irritability/severity of symptoms. This may involve your Physiotherapist suggesting or implementing a combination of:
In the long term, a graded exercise program is highly effective in alleviating symptoms and reducing the recurrence of shoulder bursitis by addressing the underlying biomechanical factors previously discussed. To develop an appropriate exercise plan, a biomechanical assessment is necessary, to understand the factors contributing to your bursitis.
Cortisone injections are a useful tool to gain a quick reduction to pain caused by bursitis however, they are often a short to medium term ‘solution’ as the underlying cause of the impingement has not been addressed. In almost all cases, where cortisone is indicated the optimal treatment would be to follow up with a course of Physiotherapy and exercise program.
Our Clinic has been classified as an essential service to the community. We assist by trying to keep people healthy as possible and out of surgeries and decrease hospital admissions. At Inertia Health Group we are working hard to keep our patients and team members as safe as possible.
Due to our strict infection control procedures we have been deemed a low risk clinic- we have all completed the government COVID -19 Infection Control Risk Course and have implemented new waiting room procedures as well as intensified our cleaning procedures completing these regularly through the day. We have also implemented a virtual health service for those who require advice or assistance and cannot attend the clinic.
We appreciate our patients doing the right thing also!
Please call us with any questions or concerns 08 8359 2022.